
Epidermolysis bullosa overview
 Fact-checked by
Fact-checked by Epidermolysis bullosa (EB) is a group of rare disorders characterized by extremely delicate skin that blisters and tears easily. People with the chronic skin condition are sometimes said to have butterfly skin because their skin is so fragile and can break with relatively minor pressure, friction, or trauma. The protective linings around the mouth, airways, and other internal parts of the body, called the mucous membranes, can also blister and develop wounds.
Most often, EB is a genetic condition caused by mutations that children inherit from one or both of their parents. Less commonly, the disease can be caused by a genetic mutation that occurs spontaneously instead of being inherited.
There are four main types of EB, each associated with different degrees of severity, complications, and long-term outlooks. Determining the type of EB a person has is a key step in diagnosis and may help guide treatment decisions.
EB is rare, with estimates indicating it may affect 25,000 to 50,000 people in the U.S.
Causes
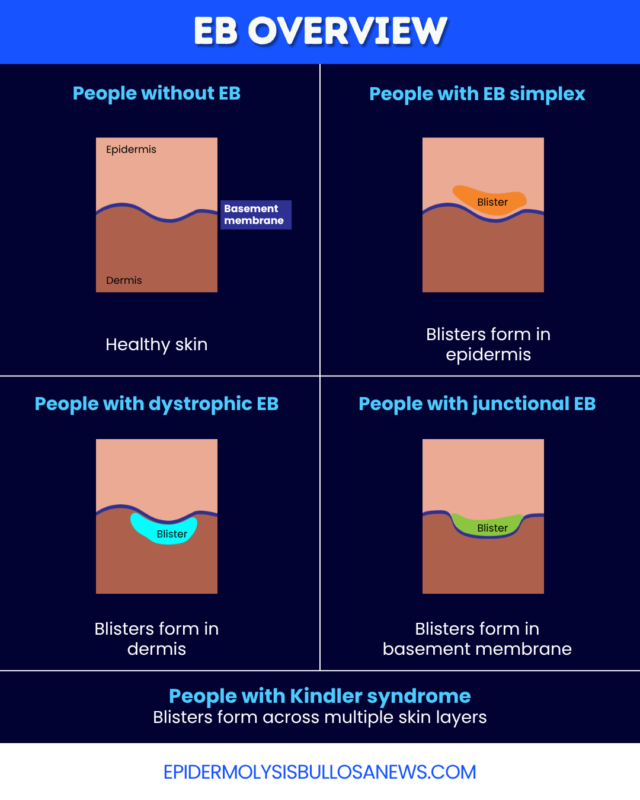
Different proteins support each of the skin’s several layers and anchor them to one another. In EB, problems with these proteins disrupt skin structure, increasing the risk of tears and blisters. Depending on the type, EB may affect the outer layer of the skin, known as the epidermis, the deeper layer underneath, called the dermis, or the structure that connects the epidermis to the dermis, which is known as the basement membrane.
The most common underlying causes of EBare mutations in the genes that contain instructions to make these structural proteins. These mutations can be:
- inherited in an autosomal dominant manner, in which a child develops EB if a mutation is inherited from one parent
- inherited via autosomal recessive inheritance, where a child only develops EB if mutations are inherited from both parents
- spontaneous, or de novo, meaning they arise randomly before birth in a person with no EB family history
Rarely, genetic mutations cannot explain EB-like symptoms. This can happen in EB acquisita (EBA), a rare autoimmune disease that causes symptoms similar to genetic forms of EB. It occurs when the immune system mistakenly attacks structural proteins of the skin, and generally arises later in life.
Types
There are four main EB types, which cause blisters to form in different skin layers:
- EB simplex (EBS): blisters form in the epidermis
- dystrophic EB (DEB): blisters form in the dermis
- junctional EB (JEB): blisters form in the basement membrane
- Kindler syndrome: blisters form in multiple skin layers
Each of these EB types is associated with mutations in genes encoding different skin structural proteins. Most of them have several subtypes that vary in severity, clinical features, inheritance pattern, and long-term outcomes.
Determining which specific type and subtype of EB a person has is key to ensuring adequate treatment, long-term monitoring, and proper care.
Signs and symptoms
All types of EB lead to extremely fragile skin that is prone to tearing and blistering. Common EB symptoms include:
- skin blistering and scarring
- skin that becomes unusually thick or thin
- skin itchiness or pain
- slow-healing or chronic wounds
- nail changes
While EB skin blistering can occur anywhere on the body, it often affects the hands, feet, elbows, knees, and other areas that experience regular friction. When it occurs on the scalp, it can cause the hair to become unusually thin, or lead to permanent hair loss.
In some subtypes, blisters may form inside the mouth or in the mucus membranes lining other internal parts of the body. This can lead to other symptoms and complications, such as difficulty swallowing and eating, which can lead to nutritional problems and growth delays.
The type and severity of EB symptoms can vary widely between individuals, depending on disease type, management strategies, and other factors.
Diagnosis
EB diagnosis usually happens in early childhood, although people with milder forms of EB may not be diagnosed until adulthood. The skin’s appearance may make doctors suspect EB, prompting more extensive testing to confirm a diagnosis and determine the disease’s type and subtype.
The process of diagnosis may entail:
- physical examination: to identify features of EB, including lesion patterns that may point toward a specific type
- genetic testing: to identify disease-causing mutations and pinpoint the disease type
- skin biopsy: to find structural abnormalities in the skin that are consistent with EB
Genetic testing is considered the gold standard for an EB diagnosis, but such tests can be time-consuming and costly. A skin biopsy, in which doctors remove and examine small samples of healthy and blistered skin, may help speed diagnosis and guide urgent care decisions in some cases. However, a skin biopsy is an invasive procedure, and it cannot identify EB’s underlying genetic cause. Biopsies may also not detect clear abnormalities in people with milder forms of the disease.
In milder cases, it can be more difficult to connect symptoms to EB, so reaching a correct diagnosis may take more time. Referral to a specialist who knows what EB is and how to manage it can help this process.
Treatment
There is no cure for EB, so treatment largely focuses on:
- protecting the skin to prevent new blisters and wounds from forming
- promoting wound healing
- easing pain, itching, and other symptoms
- preventing and managing complications
This may involve a combination of medications, home care, lifestyle changes, and other interventions.
Wound prevention strategies may include:
- wearing loose-fitting clothing that doesn’t rub the skin
- minimizing exposure to the sun and heat
- wearing protective bandages that don’t stick to the skin
Despite preventive measures, wounds can still develop, particularly in more severe cases. Proper wound care is important to promote healing and prevent complications. It may involve:
- cleaning wounded or blistered areas
- regularly changing dressings
- applying topical treatments directly on wounds to promote healing
- monitoring wounds for signs of infection
Among possible treatments are the approved EB medications Filsuvez (birch triterpenes), Vyjuvek (beremagene geperpavec-svdt), and Zevaskyn (prademagene zamikeracel).
People with EB can also experience different types of pain, including that associated with dressing changes, which may require medications or other management strategies. Modifications to home routines, like adding salt or oatmeal to baths, may also ease pain for some people.
Regular monitoring and follow-up care can help identify any signs of complications, including infected wounds, allowing for proper treatment to be started early.
Living with EB
The daily routine of monitoring, cleaning, dressing, and treating wounds can be time-consuming for patients and caregivers, especially with more severe forms of EB.
Everyday activities like bathing and dressing are often more challenging for people living with EB due to physical limitations and the constant risk of new blisters and wounds forming. Strategies to improve the quality of daily life may include:
- using adaptive or mobility devices to make everyday tasks easier
- wearing specialized shoes, socks, or clothes to reduce friction and minimize the risk of skin injury
- adding padded covers to seatbelts and steering wheels to reduce the risk of blistering caused by pressure while driving
- using soft toothbrushes to prevent tearing inside the mouth when brushing teeth
- consulting an occupational therapist to find new and safe ways to engage in daily activities
Emotional impact
EB can affect emotional well-being, as well as physical health. Some people with EB may struggle to participate in activities they enjoy or feel frustrated by the degree of their dependence on caregivers. The uncertainty of the disease course may also cause emotional distress.
More severe forms of EB are highly visible, and can affect body image and everyday relationships. Additionally, EB can cause invisible burdens, such pain and itchiness, that may go unrecognized.
Families of people with EB often also experience emotional challenges.
Having strong personal and social support networks may help promote a better quality of life for people with EB and those close to them. Care teams, community networks, and EB-focused organizations may also provide resources and support.
Outlook
The prognosis of EB varies, depending largely on the severity and type of the disease. People with milder forms of EB may have a normal or near-normal lifespan, while those with severe forms, particularly severe subtypes of JEB and recessive DEB, may have a reduced life expectancy.
Certain complications of EB can also influence prognosis. People with some types of EB, particularly DEB and JEB, are at a high risk of developing a type of skin cancer called squamous cell carcinoma, which can be life-threatening.
Regular follow-up and specialized care, including monitoring for cancer and other complications, can help improve the long-term outlook of EB.
Epidermolysis Bullosa News is strictly a news and information website about the disease. It does not provide medical advice, diagnosis, or treatment. This content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.


